Not every fibroid requires removal before IVF. But some types significantly reduce implantation rates. Here is the clinical framework that determines what needs treatment – and what can be safely left alone.
Uterine fibroids are among the most commonly diagnosed gynaecological conditions in India, affecting an estimated 20 to 40 percent of women of reproductive age. When a woman is preparing for IVF, the discovery of a fibroid on ultrasound – or the presence of an existing fibroid diagnosis – frequently raises an urgent question: does this need to be removed before I proceed with treatment?
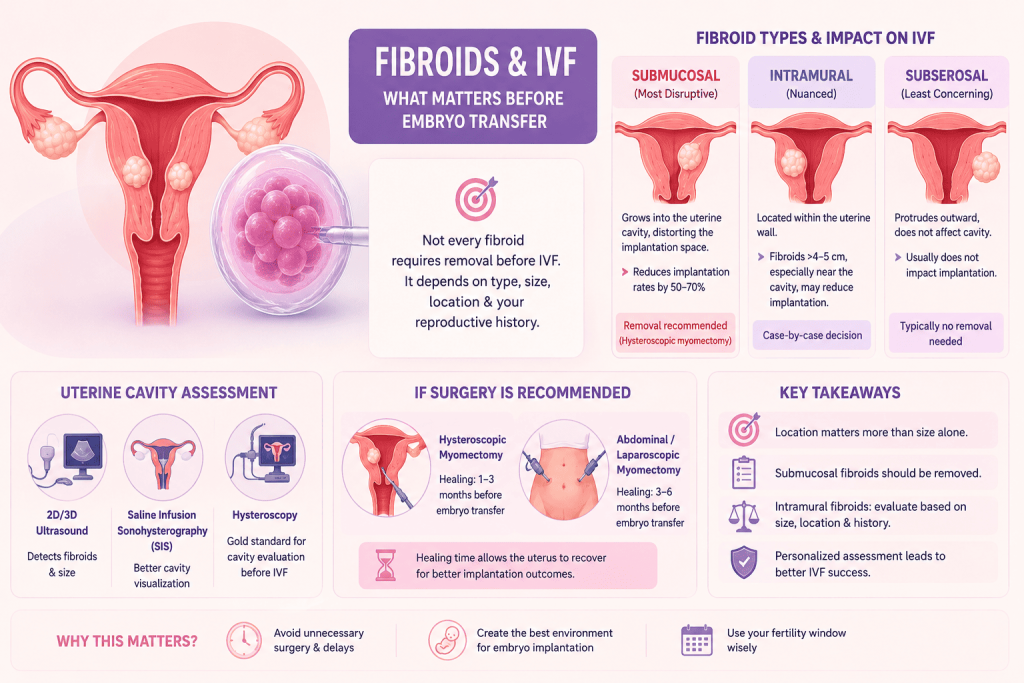
The answer is not a simple yes or no. It depends entirely on the type of fibroid, its size, its precise location within the uterine architecture, and the individual patient’s reproductive history. Understanding this distinction can mean the difference between an unnecessary surgical delay and proceeding confidently with a well-planned IVF cycle.
Understanding Fibroid Classification: Why Location Is Everything
Fibroids are classified by their relationship to the layers of the uterine wall. The three principal categories – submucosal, intramural, and subserosal – have very different implications for IVF outcomes, and it is this classification, more than size alone, that drives clinical decision-making.
Understanding Fibroid Classification: Why Location Is Everything
Submucosal fibroids grow into the uterine cavity itself, distorting or occupying the space where an embryo needs to implant. Even small submucosal fibroids – under 1 cm – have been shown in multiple studies to significantly reduce implantation and live birth rates in IVF. They are classified on a system developed by the European Society of Hysteroscopy: Type 0 (entirely within the cavity), Type 1 (more than 50 percent intracavitary), and Type 2 (less than 50 percent intracavitary). Type 0 and Type 1 fibroids carry the strongest evidence for surgical removal before embryo transfer.
Clinical consensus: Submucosal fibroids that distort the uterine cavity reduce IVF implantation rates by an estimated 50 to 70 percent. Hysteroscopic myomectomy – removal through the vaginal canal without abdominal incision – is the standard surgical approach and is associated with significant improvement in subsequent IVF outcomes.
Intramural fibroids - a nuanced picture
Intramural fibroids are contained within the muscular wall of the uterus and do not protrude into the cavity. Their impact on IVF is more contested in the medical literature. The current evidence suggests that intramural fibroids larger than 4 to 5 cm – particularly those located near the endometrial lining – are associated with reduced implantation rates and should be evaluated for removal. Smaller intramural fibroids that do not distort the cavity are generally considered acceptable to monitor rather than operate on before an IVF cycle, particularly if the patient’s age or ovarian reserve makes delaying treatment clinically costly.
The decision becomes more complex when multiple smaller intramural fibroids are present together, when they are located in the posterior wall near the cavity, or when a patient has a history of recurrent implantation failure. In these circumstances, a more aggressive pre-IVF evaluation is warranted.
Subserosal fibroids - generally the least concerning
Subserosal fibroids protrude outward from the uterus toward the pelvic cavity. Because they do not involve the uterine cavity, they are generally considered unlikely to affect embryo implantation and are typically not removed before IVF. The exception is a pedunculated subserosal fibroid – one attached by a narrow stalk – which carries a small risk of torsion and may be recommended for removal on safety rather than fertility grounds.
The Role of Uterine Cavity Assessment
Standard 2D transvaginal ultrasound is useful for detecting fibroids but may not provide the resolution needed to assess cavity involvement accurately. Before an IVF cycle, particularly in patients with known or suspected fibroids, a 3D transvaginal ultrasound or saline infusion sonohysterography (SIS) provides a significantly clearer picture of the cavity contour.
Hysteroscopy – a direct visual examination of the uterine cavity using a fine camera – remains the gold standard for evaluating the endometrial environment before IVF. For patients with a history of failed IVF cycles, unexplained implantation failure, or significant fibroid burden, diagnostic hysteroscopy should be considered a routine part of pre-cycle assessment rather than an optional add-on.
If Surgery Is Recommended: What to Expect and When to Cycle
The timing of IVF after myomectomy depends on the surgical approach and the extent of the procedure. Hysteroscopic myomectomy for submucosal fibroids typically requires a healing period of one to three months before embryo transfer. Abdominal or laparoscopic myomectomy for larger intramural fibroids may require three to six months of recovery to allow the uterine wall to heal sufficiently.
It is worth noting that myomectomy, while generally safe, does not guarantee fibroid recurrence will not occur. Younger patients with multiple fibroids at the time of surgery have a higher likelihood of recurrence. The fertility window post-surgery – particularly in women over 35 – should therefore be used efficiently, with IVF planning beginning in parallel with surgical recovery.
Fibroids and IVF: The Questions Worth Asking Your Specialist
- Has a 3D ultrasound or saline infusion sonohysterography been performed to assess cavity involvement?
- What is the exact classification and size of my fibroid?
- Is the fibroid distorting my uterine cavity?
- What does the evidence say about IVF outcomes with my specific fibroid type?
- If surgery is recommended, what is the expected recovery timeline and when can IVF proceed?
- What is the risk of fibroid recurrence and how does that affect our treatment planning?
At Nishant IVF and Fertility Centre in Jaipur, every patient with a known fibroid undergoes a thorough pre-cycle uterine. Treatment decisions are made on the basis of fibroid classification, cavity involvement, patient age, and overall fertility picture – not as a blanket protocol. In many cases, fibroids that appeared concerning on initial imaging can be confidently left in place while proceeding with IVF. In others, a short surgical step is the decisive factor between repeated failure and a successful pregnancy.
Consultation: To have your fibroid evaluated in the context of IVF planning, contact Nishant IVF at +91 99502 84285 or visit www.nishantivfcare.com
Fibroids and IVF : FAQs
No. The decision depends on the type and location of the fibroid. Submucosal fibroids that distort the uterine cavity almost always require removal before embryo transfer. Large intramural fibroids near the cavity may also need treatment. Subserosal fibroids – which protrude outward from the uterus – generally do not require removal before IVF as they are unlikely to interfere with implantation.
Research shows that submucosal fibroids distorting the uterine cavity reduce IVF implantation rates by an estimated 50 to 70 percent. Intramural fibroids larger than 4 to 5 cm may reduce success rates by 20 to 30 percent. Subserosal fibroids have minimal documented impact on IVF outcomes in most studies.
Standard 2D transvaginal ultrasound is useful for detecting fibroids but may miss subtle cavity involvement. For IVF planning, a 3D transvaginal ultrasound or saline infusion sonohysterography (SIS) provides a more accurate picture. Diagnostic hysteroscopy – a direct camera examination of the uterine cavity – remains the gold standard and can simultaneously treat any intrauterine pathology found.
After hysteroscopic myomectomy for submucosal fibroids, IVF can typically proceed within one to three months. After abdominal or laparoscopic myomectomy for larger intramural fibroids, a waiting period of three to six months is usually recommended to allow the uterine wall to heal adequately before embryo transfer.
Yes, fibroid recurrence is possible after myomectomy, particularly in younger patients and those with multiple fibroids. The likelihood of recurrence increases over time. This is why fertility specialists aim to move forward with IVF within the post-surgical window efficiently – particularly for women over 35 – rather than delaying unnecessarily.
Disclaimer: This article provides educational information about link between Fibroids and IVF and should not replace personalized medical advice. Consult with a qualified fertility specialist for proper evaluation and treatment recommendations specific to your situation.